










© 2024 Aton Center | Privacy Policy | Terms of Use | Accessibility Statement | Grievance process | California Addiction Recovery | DHCS Licenses | Sitemap
Overview:
AToN Center holds itself to the highest standard of care and is firmly rooted in the scientist-practitioner model. In an effort to provide the highest quality of service, our San Diego treatment center continuously assesses the psychological dynamics of each individual entering treatment and assesses treatment outcomes of outgoing residents. The research and leadership team at AToN Center believes in letting data drive policy, and uses only appropriate, valid, and reliable measures to assess our performance.
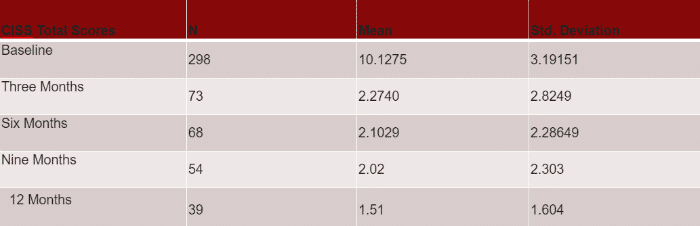
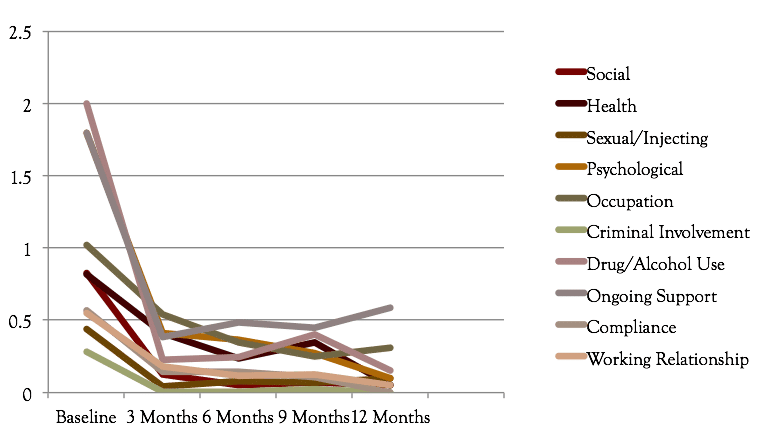
In an effort to quantify AToN Alumni progress after discharge, AToN Center contacts our Alumni at three-month intervals post-discharge. They are assessed utilizing the Christo Inventory for Substance Misuse Services (CISS) – which reviews the following domains:
- Social Functioning
- General Health
- Sexual/Injecting Risk Behavior
- Psychological
- Occupation
- Criminal Involvement
- Drug/Alcohol Use
- Ongoing Support
- Compliance
- Working Relationship
This inventory has a max of 20 points, each domain capped at 2 points. An increased score indicates increased relapse risk and distress. A “good outcome” is considered a total score of 2.9 or below. Per normative data, a score of 2.9 or below is correlated with abstinence.
This project began in October 2013. Here are our most recent results – research is ongoing!
Resident’s Urge to Use decreased significantly between weeks 1-3 in particular. Additionally, these decreases were considered a large effect when reviewing the partial eta-squared (.69).
Every single scale on the Brief Symptom Inventory demonstrated a significant decrease in symptoms from week one to week two. Five scales significantly decreased between weeks one, two and three. Finally, two scales significantly decreased every single week; and these scales were overall scales. The largest effect sizes found in the BSI were in Global Severity Index (.78), Positive Symptom Distress Index (.73), Depression (.67) and Anxiety (.64). See the below charts for further information:
- Statistically Significant in Weeks 1-4 with Partial Eta Squared
- Global Severity Index (.78)
- Positive Symptom Distress Index (.73)
- Statistically Significant in Weeks 1-3 with Partial Eta Squared
- Anxiety (.743)
- Depression .(672)
- Positive Symptom Total (.66)
- Psychosis (.608)
- Obsessive-Compulsive (.59)
- Statistically Significant in Weeks 1-2 with Partial Eta Squared
- Somatization (.64)
- Paranoia (.510)
- Hostility (.519)
- Interpersonal Sensitivity (.48)
- Phobia (.385)
Residents who attend treatment at AToN Center can reasonably expect to experience a decrease in overall symptoms on a significant level. Additionally, symptoms of depression and anxiety tend to decrease the most. For a more thorough and in-depth review, click here.
After conducting a literature review, AToN Center identified distress tolerance, coping style, and abstinence self-efficacy as important qualities that can affect treatment outcomes. In response, AToN Center implemented an assessment protocol that assessed each resident’s coping style, level of distress tolerance, and abstinence self–efficacy utilizing standardized measures. These assessments occurred within 72 hours of admission. A final assessment occurred on the resident’s final treatment day.
This data allows for an understanding of how our curriculum contributes towards improved coping styles, increased ability to tolerate distress without relapsing, and also boosts confidence in one’s ability to stay sober, which significantly can predict relapse rates. In addition, all residents at our San Diego treatment center who participated in this research were debriefed on their scores at the end of treatment in a final exit interview which provides both the client, as well as family members and other professionals with information on gains made, and areas needing focus in continued treatment.
This research was conducted over a one-year period, and 79 residents participated in the pre and post assessments. These residents on average experienced a statistically significant increase in distress tolerance in the 30 days of treatment received. Specifically, our residents demonstrated on average a 32% increase in distress tolerance from admission to discharge, taking them from a mean score of 2.56 upon entry, to a 4.16 out of a maximum 5.0. An assessment of effect size demonstrated a very large effect size (eta squared .58). Effect sizes over a .4 are statistical speak for “mathematically very significant!”
AToN Center residents also had a statistically significant increase in abstinence self-efficacy; with an average score upon admission of 2.57 “not very confident” which increases to a mean score of 4.31 which is “near extremely confident.” This scale also maxes at 5. This change represents a 35% increase in abstinence self-efficacy from admission to discharge. This effect size was also very large (eta squared .76).
AToN’s San Diego treatment center residents also subjectively reported an increase of approach coping skills, which reflect use of active coping skills, in lieu of avoidance techniques such as numbing, pretending a problem will go away on its own, and self-medicating. They also reported a decrease in using less than helpful avoidance techniques. Specifically, approach coping skills went from an “average” range to a “somewhat above average” range. Avoidant coping skills decreased from “well above average,” to “somewhat above average.” This shift from focusing on avoidant coping skills to increasing approach coping skills has been reported in research to be most effective in helping individuals prepare for success in recovery.
For a more in-depth view of the research reported above, you may consult Dr. Cannon’s Assessment of AToN Curriculum.
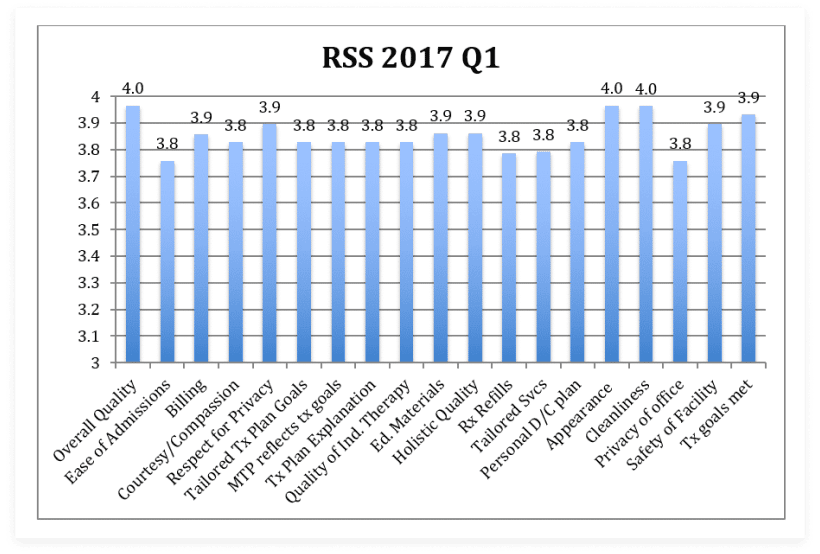
AToN Center conducts Resident Satisfaction Surveys in order to elicit feedback from our residents about how they rate different facets of our program. At the end of their stay, we ask residents to rate 19 domains on a 4-point scale. We highly value this information as it allows us to make programmatic improvements. We are happy to report that we consistently receive excellent results!
During the first Quarter of 2017, all scores ranged from 3.8 – 4.0 out of 4, representing very slight fluctuations in some categories. The lowest score (3.8) was slightly higher than our lowest score (3.5) in the fourth quarter of 2016. Across the board residents highly rated AToN Center including an average of 4’s on overall quality, appearance, and cleanliness! Generally reflected on the tool were “Excellent” and “Good” scores. Only one former resident rated one category as “Fair” and no one categorized any domain as “Poor.”
All residents (100%) this quarter would recommend AToN Center to a friend!
It is very rare to see a treatment center disclose their data on relapse rates because the numbers at first glance can seem misleading and disheartening. The truth is that the recovery pattern from substance dependence is much like that of other relapsing conditions such as diabetes, weight gain, and domestic violence victimization. These conditions often take numerous steps forward into recovery, and sometimes, they take steps backwards, known as “slips” if they are short in duration. Some cases revert to full blown relapses, which is where the individual regresses to a more severe stage of impairment.
Some social scientists, Terence Gorski being the most famous, have dramatically influenced our understanding of addiction by describing the condition of addiction or substance dependence as a “relapsing condition.” Gorski proposed that relapse can be expected as part of the condition, and is not always a “bad” thing if it leads the individual into a deeper state of understanding of their vulnerabilities, and if exploration of the underlying factors that contributed to the relapse are used to prevent harm in the future, and re-engage in supportive treatment activities.
Our goal at AToN Center is to help individuals prevent deterioration in their lives and with their health, and to assist them in restoring whatever areas of health possible; physically, relationally, spiritually, and emotionally. As consistent with recommendations from the American Psychological Association, the safest recovery approach for individuals with substance dependence is abstinence, and that is our goal.
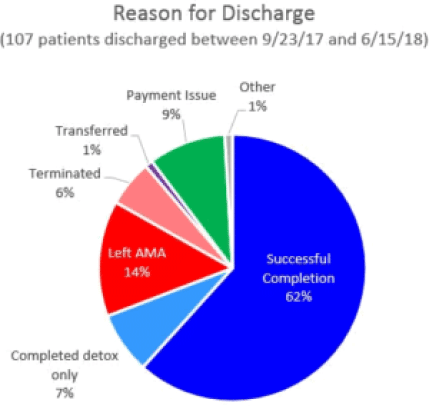
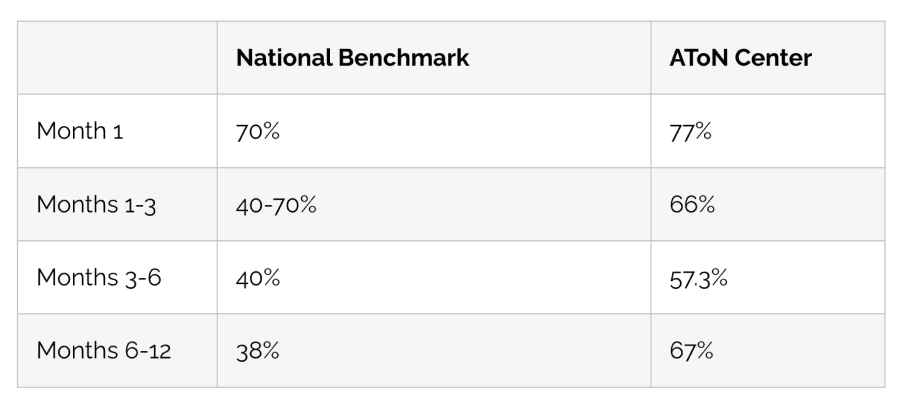
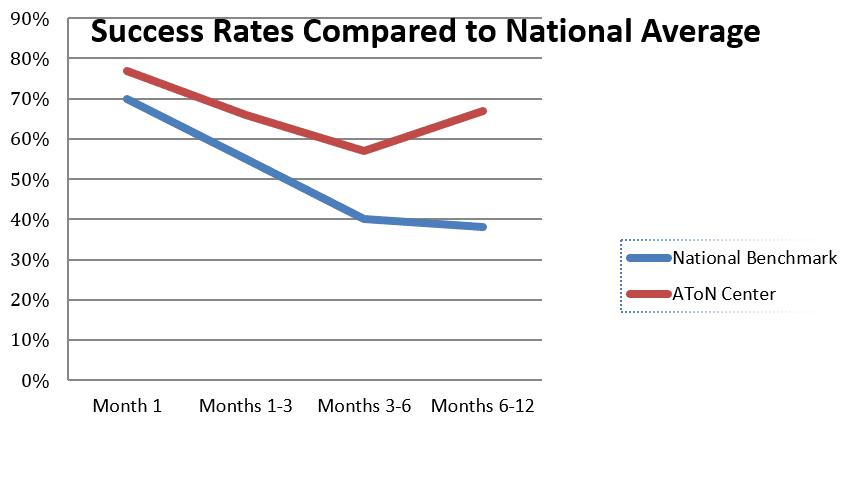
Comparison to National Benchmark
If you have ever attempted to identify success rates for the field of recovery, you know how difficult it may be! Below are AToN Center’s success rates. These rates must be interpreted with caution. To the best of AToN Center’s knowledge, these rates are accurate as possible. These rates are determined based on Aftercare outreach phone calls. Only residents who discharge with a “completed” status are afforded the benefit of Aftercare. After a period of time, some residents request to be taken off of the Aftercare outreach list.
Others have become very busy in their lives of recovery and respond to phone calls intermittently. Others have relapsed. Residents are removed from the Aftercare lists if they have requested AToN do so, or if they do not respond after several months. Therefore, these rates are based on those residents who are still receiving Aftercare phone calls. For the purposes of data analysis, all residents who are on the list, but who have not responded, are considered “relapsed.”
As with all research, we advise “buyer beware” if you come across a treatment program who is reporting long term sobriety rates at 85% and above as these would be far in excess of the treatment community standard, and such studies likely have questionable research design methods.
AToN Center recommends a thorough discharge plan for all residents inclusive of structured support for the first 90 days post-discharge, and the data emphasizes the importance of maintaining vigilance post 90 days as well. The good news is that many individuals, who report a slip or relapse, reengage with their providers and get back on track quickly.
National Benchmark Data from National Institute of Health Website:
Prochaska, J. O., DiClemente, C. C., Norcross, J. C. (1992). In search of how people change. Applications to addictive behaviors. American Psychologist, 47, 1102-1114.
AToN Center reviews the ongoing literature in our field so we can update our treatment and curriculum as our understanding of addiction progresses. While not an exhaustive list of the articles reviewed, below are some articles that have informed our current treatment curriculum. This page will be updated on a regular basis.
Adam, T. C., & Epel, E. S. (2007). Stress, eating and the reward system. Physiology & Behavior, 91(4), 449-458. doi:10.1016/j.physbeh.2007.04.011
Adamson, S. J., Sellman, J.D., & Frampton, C.M.A. (2009). Patient predictors of alcohol treatment outcome: A systematic review. Journal of Substance Abuse Treatment, 36, 75-86.
Addiction is a Chronic Disease. (n.d.). Retrieved May 09, 2017, from https://archives.drugabuse.gov/about/welcome/aboutdrugabuse/chronicdisease/
Adler, M. W., Brady, K., Brigham, G., Carroll, K. M., Clayton, R. R., Cottler, L. B., . . . Woody, G. (2012). Principles of drug addiction treatment: a research-based guide. Rockville, MD: National Institute on Drug Abuse, National Institutes of Health, U.S. Department of Health and Human Services.
Alderman, B. L., Olson, R. L., Brush, C. J., & Shors, T. J. (2016). MAP training: combining meditation and aerobic exercise reduces depression and rumination while enhancing synchronized brain activity. Translational Psychiatry, 6(2), 1-9. doi:10.1038/tp.2015.225
Anacker, C., Zunszain, P., Cattaneo, A., Carvalho, L., Thuret, S., Price, J., & Pariante, C. (2011). S.04.02 Antidepressants modulate human hippocampal neurogenesis by activating the glucocorticoid receptor. European Neuropsychopharmacology, 21, 738-750. doi:10.1016/s0924-977x(11)70246-2
Azizi, A., Borjall, A., Golzari, M. (2010). The Effectiveness of Emotion Regulation Training and Cognitive Therapy on the Emotional and Addictional Problems of Substance Abusers. Iran Journal of Psychiatry, 5(2), 60-65.
Babor, T. F., Longabaugh, R., Zweben, A. Fuller, R. K., Sout, R. L., Anton, R. F., & Randall, C. L. (1994). Issues in the definition and measurement of drinking outcomes in alcoholism treatment research. Journal of Studies on Alcohol, Supplement 12, 101-111.
Beck, A. K., Forbes, E., Baker, A. L., Kelly, P. J., Deane, F. P., Shakeshaft, A., . . . Kelly, J. F. (2017). Systematic Review of SMART Recovery: Outcomes, Process Variables, and Implications for Research. Psychology of Addictive Behaviors,31(1), 1-20.
Berenz, E. C., Kevorkian, S., Chowdhury, N., Dick, D. M., Kendler, K. S., & Amstadter, A. B. (2016). Posttraumatic stress disorder symptoms, anxiety sensitivity, and alcohol-use motives in college students with a history of interpersonal trauma. Psychology of Addictive Behaviors, 30(7), 755-763. doi:10.1037/adb0000193
Billings, A., & Moos, R. (1981). The role of coping responses and social resources in attenuating the stress of life events. Journal of Behavioral Medicine, 4, 139-157.
Billings, A., & Moos, R. (1984). Coping, stress, and social resources among adults with unipolar depression. Journal of Personality and Social Psychology, 46, 877-891.
Bowen, S., Chawla, N., Collins, S. E., Witkiewitz, K., Hsu, S., Grow, J., . . . Marlatt, A. (2009). Mindfulness-Based Relapse Prevention for Substance Use Disorders: A Pilot Efficacy Trial. Substance Abuse, 30(4), 295-305. doi:10.1080/08897070903250084
Bowen, S., & Vieten, C. (2012). A compassionate approach to the treatment of addictive behaviors: The contributions of Alan Marlatt to the field of mindfulness-based interventions. Addiction Research & Theory, 20(3), 243-249. doi:10.3109/16066359.2011.647132
Bowen, S., Witkiewitz, K., Clifasefi, S. L., Grow, J., Chawla, N., Hsu, S. H., . . . Larimer, M. E. (2014). Relative Efficacy of Mindfulness-Based Relapse Prevention, Standard Relapse Prevention, and Treatment as Usual for Substance Use Disorders. JAMA Psychiatry, 71(5), 547. doi:10.1001/jamapsychiatry.2013.4546
Brown, R.A., Lejuez, C.W., Kahler, C.W. & Strong, D.R. (2002). Distress tolerance and duration of past smoking cessation attempts. Journal of Abnormal Psychology, 111, 180-185.
Canadian Agency for Drugs and Technologies in Health – Rapid Review (2009). Naltrexone in Combination with Acamprosate for the Treatment of Alcohol Dependence: A Review of the Clinical and Cost-Effectiveness
Canadian Agency for Drugs and Technologies in Health – Rapid Review (2010). Disulfiram for Alcohol Dependence: Clinical Effectiveness and Safety
Canadian Agency for Drugs and Technologies in Health – Rapid Review: 2015. Yoga for the Treatment of Post-Traumatic Stress Disorder, Generalized Anxiety Disorder, Depression, and Substance Abuse: A Review of the Clinical Effectiveness and Guidelines
Canadian Agency for Drugs and Technologies in Health – Rapid Review: 2016. Optimal Evidence-Based Therapies for the Treatment of Addictions: Clinical Effectiveness and Guidelines
Carbonari, J.D., & DeCelemente, C.C. (2000). Using transtheoretical model of profiles to differentiate levels of alcohol abstinence success. Journal of Consulting and Clinical Psychology, 68, 810-817.
Connors, G.J., DiClemente, C.C., Velasquez, M.M. & Donovan, D.M. (2013). Substance abuse treatment and the stages of change. New York: The Guildford Press.
Coffey, S. F., Schumacher, J. A., Nosen, E., Henslee, A. M., Littlefield, A. K., Lappen, A., & Stasiewicz, P. R. (2016). Supplemental Material for Trauma-Focused Exposure Therapy for Chronic Posttraumatic Stress Disorder in Alcohol and Drug Dependent Patients: A Randomized Controlled Trial. Psychology of Addictive Behaviors. doi:10.1037/adb0000201.supp
Cooney, .L., Litt, M.D. , Cooney, J.L., Pilkey, D.T., Steinberg, H.R. & Oncken, C.A. (2007). Alcohol and tobacco cessation in alcohol dependent smokers: analysis of real-time reports. Psychology of Addictive Behaviors, 21(3), 277-286.
Daniels, A., chair. A Path Forward to Measuring Continuing Care Management for Substance Use Illness: Patient-Focused Episodes of Care. Washington, DC: National Quality Forum; 2009.
Dennhardt, A.A. & Murphy, J.G. (2011). Associations between depression, distress tolerance, delay discounting, and alcohol related problems in European American and African American College Students, Psychology of Addictive Behaviors, 25(4), 595-604.
DiClemente, C. C., Carbonari, J.P., Montgomery, R.P.G. & Hughes, S.O. (1994). The alcohol abstinence self-efficacy scale, The Journal of Studies on Alcohol and Drugs, 55, 141-148.
Dimeff, L. (2008). Dialectical Behavior Therapy for Substance Abusers. Addiction Science & Clinical Practice, 4(2), 39-47. doi:10.1151/ascp084239. Retrieved from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2797106/
Evidence-based practice in psychology. (2006). American Psychologist, 61(4), 271-285. doi:10.1037/0003-066x.61.4.271
Fein, G. and Cardenas, V.A. (2015). Improving Health Through Translational Alcohol Research: Neuroplasticity in human alcoholism: Studies of extended abstinence with potential treatment implications. The Journal of the National Institute on Alcohol Abuse and Alcoholism. Vol. 37, No. 1, Pages 125-141.
Fisher, J. E., & O’Donohu, W. T. (n.d.). Practitioner’s Guide to Evidence Based Psychotherapy. Springer. doi:1007/978-0-387-28370-8
Greenfield, B.L., Venner, K.L., Kelly, J.F., Slaymaker, V. & Bryan, A.D. (2012) The impact of depression on abstinence self – efficacy and substance use outcomes among emerging adults in residential treatment. Psychology of Addictive Behaviors, 26(2), 246-254.
Greenfield, S.F., Weiss, R.D., Muenz L.R., Vagge, L.M., Kelly, J.F., Bello, L.R., & Michael, J. (1998). The effect of depression on return to drinking: A prospective study. Archives of General Psychiatry, 55, 259-265.
Hardman, RJ, Kennedy, G, Macpherson H, Scholey, AB, & Pipingas, A (2016). Adherence to a Mediterranean-Style Diet and Effects on Cognition in Adults: A Qualitative Evaluation and Systematic Review of Longitudinal and Prospective Trials, Frontiers in Nutrition, Jul 2016, vol. 3, article 22.
Harris, A. H., Kivlahan, D., Barnett, P. G., & Finney, J. W. (2011). Longer Length of Stay Is Not Associated with Better Outcomes in VHA’s Substance Abuse Residential Rehabilitation Treatment Programs. The Journal of Behavioral Health Services & Research, 39(1), 68-79. doi:10.1007/s11414-011-9250-2
Harrison, L. D., & Hughes, A. (1997). The validity of self-reported drug use: improving the accuracy of survey estimates. Rockville, MD: U.S. Dept. of Health and Human Services, National Institutes of Health, National Institute on Drug Abuse, Division of Epidemiology and Prevention Research.
Hayes, S., Strosahl, K., Wilson, K. (2011). Acceptance and Commitment Therapy, Second Edition: The Process and Practice of Mindful Change, Edition 2. New York, NY: Gilford Press.
Hayes, S. C., Wilson, K. G., Gifford, E. V., Bissett, R., Piasecki, M., Batten, S. V., . . . Gregg, J. (2004). A Preliminary trial of twelve-step facilitation and acceptance and commitment therapy with polysubstance-abusing methadone-maintained opiate addicts. Behavior Therapy, 35(4), 667-688. doi:10.1016/s0005-7894(04)80014-5
Holt, L.J., Litt, M.D. & Cooney, N.L. (2012). Prospective analysis of early lapse to drinking and smoking among individuals in concurrent alcohol and tobacco treatment. Psychology of Addictive Behaviors, 26(3), 561-572.
Houben K., Wiers R. W., Jansen A. (2011b). Getting a grip on drinking behavior: training working memory to reduce alcohol abuse. Psychol. Sci. 22, 968–975. 10.1177/0956797611412392
Hölzel, B. K., Carmody, J., Vangel, M., Congleton, C., Yerramsetti, S. M., Gard, T., & Lazar, S. W. (2011). Mindfulness practice leads to increases in regional brain gray matter density. Psychiatry Research: Neuroimaging, 191(1), 36-43. doi:10.1016/j.pscychresns.2010.08.006
Horvath, AT. (2003). Sex, Drugs, Gambling & Chocolate: A Workbook for Overcoming Addictions. Impact Publishers
Huebner, R.B., Kantor L.W. (2011). Expanding the Framework of Treatment: Advances in alcoholism treatment. The Journal of the National Institute on Alcohol Abuse and Alcoholism. Vol. 33, No. 4, Pages 295-299.
Hser, Y.-I., Evans, E., Huang, D., & Anglin, D. M. (2004). Relationship between drug treatment services, retention and outcomes. Psychiatric Services, 55 (7), 767-774.
Ilgen, M., McKellar, J. & Moos, R. (2007). Personal and treatment related predictors of abstinence self – efficacy. Journal of Studies on Alcohol and Drugs, 68(1), 126-132.
Ilgen, M., McKellar, J & Tiet, Q. (2005). Abstinence self – efficacy and abstinence 1 year after substance use disorder treatment. Journal of Consulting and Clinical Psychology, 73(6), 1175-1180.
Institute for Behavior and Health Addiction Treatment Outcomes Working Group. (2014). Creating a new standard for addiction treatment outcomes. Institute for Behavior and Health. Rockville, MD.: A Report of the Institute for Behavior and Health.
Kelly, J.F. and Yeterian, J.D. (2011). Expanding the Framework of Treatment: The role of mutual-help groups in extending the framework of treatment. The Journal of the National Institute on Alcohol Abuse and Alcoholism. Vol. 33, No. 4, Pages 350-355.
Kiefer, F., Vollstädt-Klein, S., Loeber, S., Kirsch, M., Richter, A., & Mann, K. (2011). P.6.a.003 Effect of cue-exposure based training in alcoholics on fMRI cue-reactivity. European Neuropsychopharmacology, 21. doi:10.1016/s0924-977x(11)70914-2
Kjaer, T. W., Bertelsen, C., Piccini, P., Brooks, D., Alving, J., & Lou, H. C. (2002). Increased dopamine tone during meditation-induced change of consciousness. Cognitive Brain Research, 13(2), 255-259. doi:10.1016/s0926-6410(01)00106-9
Kleber, H.D., Weiss, R.D., Anton, R.F., George, T.P., Greenfield, S.F., Kosten, T.R., O’Brien, C.P., Rounsaville, B.J., Strain, E.C., Ziedonis, D.M., Hennessy, G., Connery, H.S. (2010). Practice Guideline for the Treatment of Patients With Substance Use Disorders, Second Edition. (n.d.). APA Practice Guidelines for the Treatment of Psychiatric Disorders: Comprehensive Guidelines and Guideline Watches. doi:10.1176/appi.books.9780890423363.141077
Lazar, S. W., Kerr, C. E., Wasserman, R. H., Gray, J. R., Greve, D. N., Treadway, M. T., . . . Fischl, B. (2005). Meditation experience is associated with increased cortical thickness. NeuroReport, 16(17), 1893-1897. doi:10.1097/01.wnr.0000186598.66243.19
Lazarus, R. (1991). Cognition and motivation in emotion. American Psychologist, 46, 352-367.
Lee EB, An W, Levin ME, Twohig MP. An initial meta-analysis of Acceptance and Commitment Therapy for treating substance use disorders. Drug Alcohol Depend. 2015 Oct 1;155:1-7.
Levin, C., Ilgen, M. & Moos, R. (2007). Avoidance coping strategies moderate the relationship between self – efficacy and 5 year alcohol treatment outcomes.
Linehan, M. (1993). Cognitive-Behavioral Treatment of Borderline Personality Disorder. New York, NY: Guilford Publications, Inc.
Linehan, M. (2015). DBT Skills Training Handouts and Worksheets. New York, NY: The Guilford Press.
Linehan, M. (2015). DBT Skills Training Manual, Second Edition. New York, NY: The Guilford Press.
Locke, E.A., & Latham, G.P. (1990). A theory of goal setting and task performance. Englewood Cliffs, NJ: Prentice-Hall.
Locke, E. A., & Latham, G. P. (2002). Building a practically useful theory of goal setting and task motivation: A 35-year odyssey. American Psychologist, 57(9), 705-717. doi:10.1037/0003-066x.57.9.705
Longabaugh, R., Mattson, M. E., Connors, G. J., & Cooney, N. L. (1994). Quality of life as an outcome variable in alcoholism treatment research. Journal of Studies on Alcohol Supplement, 12, 119-129.
Longo, D. L., Volkow, N. D., Koob, G. F., & Mclellan, A. T. (2016). Neurobiologic Advances from the Brain Disease Model of Addiction. New England Journal of Medicine, 374(4), 363-371. doi:10.1056/nejmra1511480
Magidson, J. F., Robustelli, B. L., Seitz-Brown, C. J., & Whisman, M. A. (2017). Activity enjoyment, not frequency, is associated with alcohol-related problems and heavy episodic drinking. Psychology of Addictive Behaviors, 31(1), 73-78. doi:10.1037/adb0000220
Manuel, J. K., Hagedorn, H. J., & Finney, J. W. (2011). Implementing evidence-based psychosocial treatment in specialty substance use disorder care. Psychology of Addictive Behaviors, 25(2), 225-237. doi:10.1037/a0022398
Marlatt, G. A., & Donovan, D. M. (2008). Relapse prevention: maintenance strategies in the treatment of addictive behaviors (2nd ed.). New York: Guilford.
Miller, M. B., Dibello, A. M., Lust, S. A., Meisel, M. K., & Carey, K. B. (2017). Impulsive personality traits and alcohol use: Does sleeping help with thinking? Psychology of Addictive Behaviors, 31(1), 46-53. doi:10.1037/adb0000241
Miller, S.D., Lee, M.L., Plum, W. and Hubble, M.A. (2005). “Making Treatment Count: Client-Directed, Outcome-Informed Clinical Work with Problem Drinkers.” Psychotherapy in Australia, 2(4), 42-56.
McLellan, A. T., Lewis, D. C., O’Brien, C. P., & Kleber, H. D. (2000). Drug dependence, a chronic medical illness: Implications for treatment, insurance, and outcomes evaluation. The Journal of the American Medical Association, 284(13), 1689-1695.
Moos, R.H. (1993). Coping Responses Inventory – Professional Manual. Psychological Assessment Resources, Inc.
Moos, R., Brennan, P., Fondacaro, M., & Moos, B. (1990). Approach and avoidance coping responses among older problem and nonproblem drinkers. Psychology and Aging, 5, 31-40.
Moos, R., Finney, J. & Chan, D. (1981). The process of recovery from alcoholism: I. Comparing alcoholic patients and matched community controls. Journal of Studies on Alcohol, 42, 383-402.
Moos, .R.H., & Moos, B.S. (2006). Rates and predictors of relapse after natural and treated remission from alcohol use disorders. Addiction, 101, 212-222.
Moser & Annis (2002). The role of coping in relapse crisis outcome: a prospective study of treated alcoholics. Addiction, 91(8), 1101-1114.
Nadel, E. L., & Thornberry, T. P. (2017). Intergenerational consequences of adolescent substance use: Patterns of homotypic and heterotypic continuity. Psychology of Addictive Behaviors, 31(2), 200-211. doi:10.1037/adb0000248
Naqvi, N.H. & Morgenstern, J. (2015). Cognitive Neuroscience Approaches to Understanding Behavior Change in Alcohol Use Disorder Treatments. Alcohol Research Current Reviews, 37(1), 29-38.
Potenza, MN, Sofuoglu, M, Carroll, K., and Rounsaville, BJ (2011). Neuroscience of Behavioral and Pharmacological Treatment for Addictions, Neuron, 69, Feb 24, p. 695
Power EJ, Nishimi RY, Kizer KW, editors. Evidence-Based Treatment Practices for Substance Use Disorders. Washington, DC: National Quality Forum; 2005
Prochaska JO, DiClemente CC. Stages and processes of self change in smoking: Toward an integrative model of change. J Consult Clin Psychol 1983; 5: 390–395.
Prochaska, J. O., DiClemente, C. C., Norcross, J. C. (1992). In search of how people change. Applications to addictive behaviors. American Psychologist, 47, 1102-1114
Prochaska, J. O., Norcross, J. C., & DiClemente, C. C. (1994). Changing for good: the revolutionary program that explains the six stages of change and teaches you how to free yourself from bad habits. New York: W. Morrow.
Prochaska, J. O., & Velicer, W. F. (1997). The Transtheoretical Model of Health Behavior Change. American Journal of Health Promotion, 12(1), 38-48. doi:10.4278/0890-1171-12.1.38
Project MATCH: Hypotheses, Results, and Causal Chain Analyses, R. Longabaugh and P.W. Wirtz, editors (2001). NIH Publication No. 01–4238.
Quanbeck, A., Chin, M-Y, Isham, A., Johnson, R., Gustafson, D. (2014). Mobile Delivery of Treatment for Alcohol Use Disorders. Alcohol Research Current Reviews, 36(1), 111-122.
Rouse, B. A., Kozel, N. J., & Richards, L. G. (1995). Self-report methods of estimating drug use: meeting current challenges to validity. Springfield (Virginia): National Technical Information Service.
Sagi, Y., Tavor, I., Hofstetter, S., Tzur-Moryosef, S., Blumenfeld-Katzir, T., & Assaf, Y. (2012). Learning in the Fast Lane: New Insights into Neuroplasticity. Neuron,73(6), 1195-1203. doi:10.1016/j.neuron.2012.01.025
SAMHSA. (n.d.). Retrieved May 08, 2017, from http://nrepp.samhsa.gov/landing.aspx
SAMHSA. (n.d.). Retrieved May 08, 2017, from https://www.samhsa.gov/capt/practicing-effective-prevention/prevention-behavioral-health/adverse-childhood-experiences
Scullin, M. K., & Bliwise, D. L. (2015). Sleep, Cognition, and Normal Aging. Perspectives on Psychological Science, 10(1), 97-137. doi:10.1177/1745691614556680
Seo, D. and Sinha, R. (2015). Improving Health Through Translational Alcohol Research: Neuroplasticity and predictors of alcohol recovery. The Journal of the National Institute on Alcohol Abuse and Alcoholism. Vol. 37, No. 1, Pages 143-152.
Simons, J.S. & Gaher, R.M. (2005). The Distress tolerance scale: Development and validation of a self-report measure. Motivation and Emotion, (29)2, 83-102.
Simons, R. M., Simons, J. S., Olson, D., Baugh, L., Magnotta, V., & Forster, G. (2016). Posttraumatic stress and alcohol use among veterans: Amygdala and anterior cingulate activation to emotional cues. Psychology of Addictive Behaviors, 30(7), 720-732. doi:10.1037/adb0000200
Singer, G. H., Kim, J., Lam, Y. W., Wang, M., & Oliver, K. (2016). Psychoeducational Group Programs as Evidence-Based Practices. Supporting Families of Children With Developmental Disabilities, 25-72. doi:10.1093/acprof:oso/9780199743070.003.0002
Tonigan, J. S., Mccallion, E. A., Frohe, T., & Pearson, M. R. (2017). Lifetime Alcoholics Anonymous attendance as a predictor of spiritual gains in the Relapse Replication and Extension Project (RREP). Psychology of Addictive Behaviors, 31(1), 54-60. doi:10.1037/adb0000235
Vujanovic, A. A., Bonn-Miller, M. O., & Petry, N. M. (2016). Co-occurring posttraumatic stress and substance use: Emerging research on correlates, mechanisms, and treatments—Introduction to the special issue. Psychology of Addictive Behaviors, 30(7), 713-719. doi:10.1037/adb0000222
White, M.L. (2012). Recovery/Remission from Substance Use Disorders: An Analysis of Reported Outcomes in 415 Scientific Reports, 1868-2011 Published by the Philadelphia Department of Behavioral Health and Intellectual disAbility Services and the Great Lakes Addiction Technology Transfer Center.
White, W.L. & McLellan, A.T. (2008). Addiction as a chronic disease: Key messages for clients, families and referral sources. Counselor, 9(3), 24-33.
Wilson, K. G., & Byrd, M. R. (2004). Acceptance and Commitment Therapy for Substance Abuse and Dependence. In S. C. Hayes & K. Strosahl (Eds.), A Practical Guide to Acceptance and Commitment Therapy (pp. 153-184). New York: Springer Press.
Witkiewitz, . (2011). Predictors of heavy drinking during and following treatment. Psychology of Addictive Behaviors, 25(3), 426-438.
Witkiewitz, K., Bowen, S., Douglas, H., & Hsu, S. H. (2013). Mindfulness-based relapse prevention for substance craving. Addictive Behaviors, 38(2), 1563-1571. doi:10.1016/j.addbeh.2012.04.001
Witkiewitz, K., Donovan, D.M. & B.H. (2012). Drink refusal training as part of a combined behavioral intervention: effectiveness and mechanisms of change. Journal of Consulting and Clinical Psychology, 80(3), 440-449.
Witkiewitz, K., Lustyk, M. K., & Bowen, S. (2013). Retraining the addicted brain: A review of hypothesized neurobiological mechanisms of mindfulness-based relapse prevention. Psychology of Addictive Behaviors, 27(2), 351-365. doi:10.1037/a0029258
Witkiewitz, K., Marlatt, G.A. (2011). Expanding the Framework of Treatment: Behavioral therapy across the spectrum. The Journal of the National Institute on Alcohol Abuse and Alcoholism, Vol. 33, No. 4, Pages 313-319.
Zvolensky, M.., Marshall, E.R., Johnson, K., Hogan, J.H., Bernstein, A., Bonn-Miller, M.O. (2009). Relations between anxiety sensitivity, distress tolerance and fear reactivity to bodily sensations to coping and conformity marijuana use motives among young adult marijuana users, Experimental and Clinical Psychopharmacology, 17(1), 31-42.